
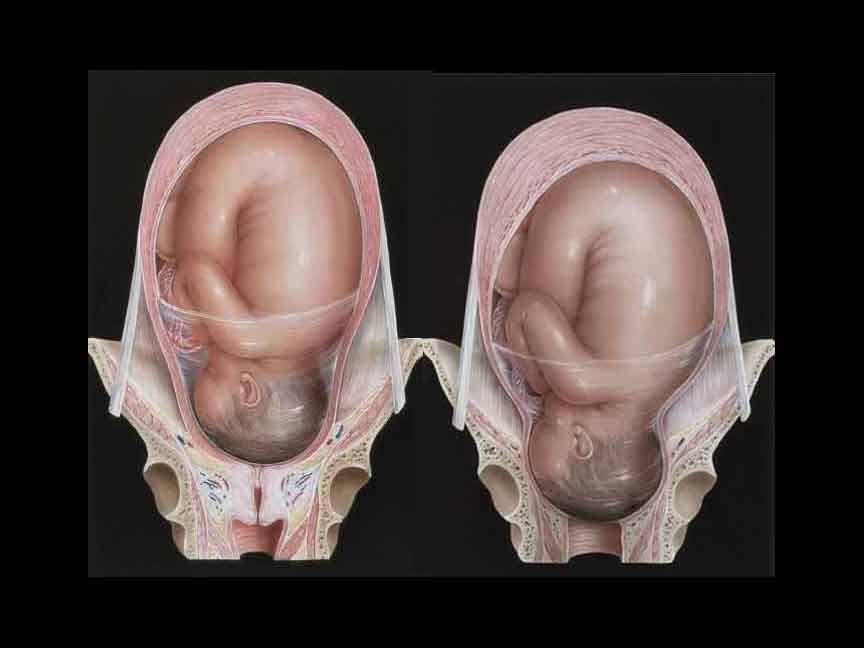
The World Health Organization (WHO) this week announced that cervical dilation is inaccurate in identifying women at risk of adverse birth outcomes. This is part of the new recommendations issued this week to establish global care standards for healthy pregnant women and reduce unnecessary medical interventions.
The new WHO guideline recognizes that every labour and childbirth is unique and that the duration of the active first stage of labour varies from one woman to another. In a first labour, it usually does not extend beyond 12 hours. In subsequent labours it usually does not extend beyond 10 hours.
To reduce unnecessary medical interventions, the WHO guideline states that the previous benchmark for cervical dilation rate at 1 cm/hr during the active first stage of labour (as assessed by a partograph or chart used to document the course of a normal labour) may be unrealistic for some women and is inaccurate in identifying women at risk of adverse birth outcomes. The guideline emphasizes that a slower cervical dilation rate alone should not be a routine indication for intervention to accelerate labour or expedite birth.

The World Health Organization (WHO) this week announced that cervical dilation is inaccurate in identifying women at risk of adverse birth outcomes. This is part of the new recommendations issued this week to establish global care standards for healthy pregnant women and reduce unnecessary medical interventions.
The new WHO guideline recognizes that every labour and childbirth is unique and that the duration of the active first stage of labour varies from one woman to another. In a first labour, it usually does not extend beyond 12 hours. In subsequent labours it usually does not extend beyond 10 hours.
To reduce unnecessary medical interventions, the WHO guideline states that the previous benchmark for cervical dilation rate at 1 cm/hr during the active first stage of labour (as assessed by a partograph or chart used to document the course of a normal labour) may be unrealistic for some women and is inaccurate in identifying women at risk of adverse birth outcomes. The guideline emphasizes that a slower cervical dilation rate alone should not be a routine indication for intervention to accelerate labour or expedite birth.
The World Health Organization (WHO) this week announced that cervical dilation is inaccurate in identifying women at risk of adverse birth outcomes. This is part of the new recommendations issued this week to establish global care standards for healthy pregnant women and reduce unnecessary medical interventions.
The new WHO guideline recognizes that every labour and childbirth is unique and that the duration of the active first stage of labour varies from one woman to another. In a first labour, it usually does not extend beyond 12 hours. In subsequent labours it usually does not extend beyond 10 hours.
To reduce unnecessary medical interventions, the WHO guideline states that the previous benchmark for cervical dilation rate at 1 cm/hr during the active first stage of labour (as assessed by a partograph or chart used to document the course of a normal labour) may be unrealistic for some women and is inaccurate in identifying women at risk of adverse birth outcomes. The guideline emphasizes that a slower cervical dilation rate alone should not be a routine indication for intervention to accelerate labour or expedite birth.
The World Health Organization (WHO) this week announced that cervical dilation is inaccurate in identifying women at risk of adverse birth outcomes. This is part of the new recommendations issued this week to establish global care standards for healthy pregnant women and reduce unnecessary medical interventions.
The new WHO guideline recognizes that every labour and childbirth is unique and that the duration of the active first stage of labour varies from one woman to another. In a first labour, it usually does not extend beyond 12 hours. In subsequent labours it usually does not extend beyond 10 hours.
To reduce unnecessary medical interventions, the WHO guideline states that the previous benchmark for cervical dilation rate at 1 cm/hr during the active first stage of labour (as assessed by a partograph or chart used to document the course of a normal labour) may be unrealistic for some women and is inaccurate in identifying women at risk of adverse birth outcomes. The guideline emphasizes that a slower cervical dilation rate alone should not be a routine indication for intervention to accelerate labour or expedite birth.
The World Health Organization (WHO) this week announced that cervical dilation is inaccurate in identifying women at risk of adverse birth outcomes. This is part of the new recommendations issued this week to establish global care standards for healthy pregnant women and reduce unnecessary medical interventions.
The new WHO guideline recognizes that every labour and childbirth is unique and that the duration of the active first stage of labour varies from one woman to another. In a first labour, it usually does not extend beyond 12 hours. In subsequent labours it usually does not extend beyond 10 hours.
To reduce unnecessary medical interventions, the WHO guideline states that the previous benchmark for cervical dilation rate at 1 cm/hr during the active first stage of labour (as assessed by a partograph or chart used to document the course of a normal labour) may be unrealistic for some women and is inaccurate in identifying women at risk of adverse birth outcomes. The guideline emphasizes that a slower cervical dilation rate alone should not be a routine indication for intervention to accelerate labour or expedite birth.
The World Health Organization (WHO) this week announced that cervical dilation is inaccurate in identifying women at risk of adverse birth outcomes. This is part of the new recommendations issued this week to establish global care standards for healthy pregnant women and reduce unnecessary medical interventions.
The new WHO guideline recognizes that every labour and childbirth is unique and that the duration of the active first stage of labour varies from one woman to another. In a first labour, it usually does not extend beyond 12 hours. In subsequent labours it usually does not extend beyond 10 hours.
To reduce unnecessary medical interventions, the WHO guideline states that the previous benchmark for cervical dilation rate at 1 cm/hr during the active first stage of labour (as assessed by a partograph or chart used to document the course of a normal labour) may be unrealistic for some women and is inaccurate in identifying women at risk of adverse birth outcomes. The guideline emphasizes that a slower cervical dilation rate alone should not be a routine indication for intervention to accelerate labour or expedite birth.
The World Health Organization (WHO) this week announced that cervical dilation is inaccurate in identifying women at risk of adverse birth outcomes. This is part of the new recommendations issued this week to establish global care standards for healthy pregnant women and reduce unnecessary medical interventions.
The new WHO guideline recognizes that every labour and childbirth is unique and that the duration of the active first stage of labour varies from one woman to another. In a first labour, it usually does not extend beyond 12 hours. In subsequent labours it usually does not extend beyond 10 hours.
To reduce unnecessary medical interventions, the WHO guideline states that the previous benchmark for cervical dilation rate at 1 cm/hr during the active first stage of labour (as assessed by a partograph or chart used to document the course of a normal labour) may be unrealistic for some women and is inaccurate in identifying women at risk of adverse birth outcomes. The guideline emphasizes that a slower cervical dilation rate alone should not be a routine indication for intervention to accelerate labour or expedite birth.
The World Health Organization (WHO) this week announced that cervical dilation is inaccurate in identifying women at risk of adverse birth outcomes. This is part of the new recommendations issued this week to establish global care standards for healthy pregnant women and reduce unnecessary medical interventions.
The new WHO guideline recognizes that every labour and childbirth is unique and that the duration of the active first stage of labour varies from one woman to another. In a first labour, it usually does not extend beyond 12 hours. In subsequent labours it usually does not extend beyond 10 hours.
To reduce unnecessary medical interventions, the WHO guideline states that the previous benchmark for cervical dilation rate at 1 cm/hr during the active first stage of labour (as assessed by a partograph or chart used to document the course of a normal labour) may be unrealistic for some women and is inaccurate in identifying women at risk of adverse birth outcomes. The guideline emphasizes that a slower cervical dilation rate alone should not be a routine indication for intervention to accelerate labour or expedite birth.
Related posts:
 CBN queries banks over inaccurate data on FOREX
CBN queries banks over inaccurate data on FOREX
 PDP warns members against identifying with splinter group
PDP warns members against identifying with splinter group
 NCAA warns pilots, airline operators against adverse weather conditions
NCAA warns pilots, airline operators against adverse weather conditions
 8,439 Nigerians experience mild, adverse effects after vaccination – NPHCDA
8,439 Nigerians experience mild, adverse effects after vaccination – NPHCDA
 Ekiti first lady charges health workers, women on free cervical cancer screening
Ekiti first lady charges health workers, women on free cervical cancer screening
 Women, Girls urged to undergo Cervical Cancer Screening
Women, Girls urged to undergo Cervical Cancer Screening
 Cervical Cancer: Why are women dying unnecessary deaths from preventable disease?
Cervical Cancer: Why are women dying unnecessary deaths from preventable disease?
 Bystander defibrillator use tied to better cardiac arrest outcomes
Bystander defibrillator use tied to better cardiac arrest outcomes



{kind=link}